



There are various well-known myths about decision aids used in the clinical encounter. One of the most persistent one is the myth that decision aids extend the clinical encounter.
Decisions aids are critical to the success of shared decision-making and self-management support. The past ten years have seen a growth in the production of decision aids, yet implementation in practice and use in clinical encounters is lagging. Despite well-established evidence, barriers remain to the introduction of decision aids; one of the most persistent argument is that decision aids extend the clinical encounter.
Decision aids are crucial to patient involvement and shared decision-making, whether applied to clinical interventions or self-management interventions. They potentially have a lasting impact on people´s life by providing unbiased information on alternative therapeutic of lifestyle choices. In COMPAR-EU we are currently reviewing the evidence on self-management interventions for Type 2 Diabetes, Obesity, Heart Failure and COPD. Based on the research, COMPAR-EU will develop decision aids, including patient decision aids, Interactive Summary of Findings tables and Evidence to Decision Frameworks. The overall aim is to build the foundation that these decision aids can be used by patients, clinicians, managers, HTA experts and industrial partners, such as IT developers. The question is, will our tools ever be implemented in practice?
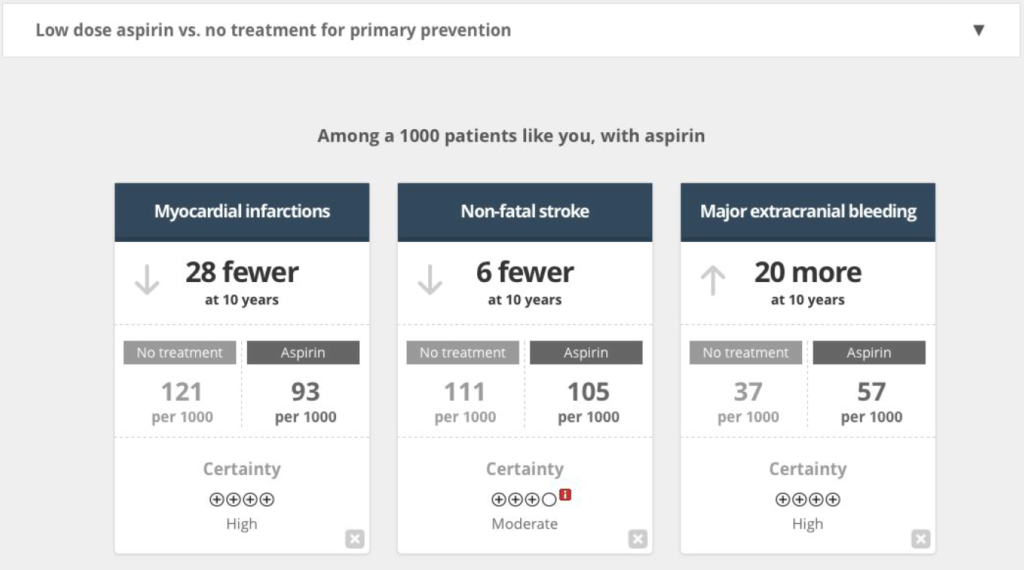
Illustration of a decision aid from the MAGIC Project
The effect of decision aids on consultation length
A major barrier to implementing decision aids is a clinician´s perception that it will extend his or her limited consultation time. In a recent systematic review, Dobler et al assess the evidence addressing this myth! Out of the 13 studies included in their review, in 9 consultation time was not significantly different in the group that used a decision aid compared to the group without. In three studies, consultation time was somewhat longer, while in one study the consultation time even decreased with the use of a decision aid. More importantly, in a study that evaluated why clinicians didn´t use a decision aid, 38.5% of clinicians said they didn´t use it for fear of extending consultation time.
The results of the review clearly don´t support the myth that decision aids extend the clinical encounter. However, what is true is that the effect of decision aids on consultation length is variable and may depend both on patient (such as health literacy level) and system level factors (such as quality of the decision aid or IT support for the decision aid). The research also shows that there are learning curves, with clinicians overcoming initial concerns after using decision aids and patients becoming more familiar with such tools, too. At the same time, arguably the quality of decision aids has improved in the last decade.

Dr Oliver Groene
Dr Oliver Groene has a track record in conducting research on patient-centred care and promoting health care systems aligned with patients´ and citizens´ needs. In the COMPAR-EU project he acts as Innovation lead to ensure that the research can be successfully integrated into health care practice to the benefit of patients, clinicians and systems.
The myth is busted – decision aids do not extend consultation time!
However, we do need to continue to work closely with patients, clinicians, managers and IT companies to ensure that decision aids are used at the right time and for the right patient. Eventually, informed decisions are crucial to improve today´s health systems, in particular with regard to the challenge of managing chronic diseases and supporting patient´s self-management.